

Knee Replacement Implants
Total Knee Implants
A total knee replacement is basically a curved metal cap on the end of the femur (thigh bone) and a flat metal tray on the top of the tibia (shin bone) with a piece of polyethylene (i.e. plastic) that sits between the two pieces of metal.
Implant fixation is mostly done with bone cement (95% of the market), but press fit implants have been gaining in popularity.
Knee replacement kinematics is a balance between letting the knee ligaments dictate the knee motion versus allowing the knee implant to force the knee motion to do what the surgeon thinks is best. Surgeons who believe the native ligaments should guide the knee motion consider a knee replacement as a knee resurfacing operation. Surgeons who believe the implant should dictate the knee motion consider a knee replacement as a knee reconstruction operation. Are we striving to mimic the original knee kinematics or create a new type of knee kinematics? These questions remain openly debated and still unanswered in the orthopedic community today
Total knee replacements can be divided into 5 groups.
Cruciate Retaining (CR)
Cruciate Sacrificing (CS)
Cruciate Substituting - Posterior Stabilized (PS)
Constrained devices
Hinged Knee Replacements

Cruciate Retaining (CR) Knee Implants
CR knee implants are thought of more as of a knee resurfacing than a knee reconstruction. CR knee implants rely on the posterior cruciate ligament to help stabilize the knee joint and help with femoral roll back. CR knee implants typically require more precise ligament balancing, feel more natural with less mechanical noises, but on average obtain slightly less knee flexion.

Cruciate Substituting (CS) Knee Implants
Cruciate Substituting (CS) knee implants remove the posterior cruciate ligament (PCL) but make up for the PCL with a very congruent medial articulating surfacing. The curvature of the medial femoral condyle is typically a single radius and matched with the curvature of the medial polyethylene (ball and socket configuration) which provides good stability, allows flexion and extension, but prevents anterior and posterior translation. The lateral side is typically unconstrained and allowed to freely move especially in the anterior to posterior direction. CS implants are sometimes called medial pivot knee replacements since the medial side does not roll back, but the lateral side does roll back.

Posterior Stabilized (PS) Knee Implants
Posterior Stabilized (PS) knee implants are thought of more as a knee reconstruction than a knee resurfacing. The posterior cruciate ligament is removed with this design. PS implants have a polyethylene post on the tibial insert that engages the femoral cam (bar in the back of the femoral component) in deep flexion. PS knees are typically easier to implant, don’t require as precise ligament balancing, obtain greater flexion, but feel more artificial since patients can feel the post engage the cam in deep flexion.
Comparison of CR vs. PS
The CR implant on the left has a simpler design and relies on the posterior cruciate ligament (shown in pink) to help with femoral roll back. The PS implant on the right has a cam (blue) and post (yellow) design that engages in deep flexion and drives femoral roll back.


Constrained Knee Implants
Constrained knee implants are used in revision settings. These implants accept stem attachments that allow fixation into the femoral and tibial diaphysis (i.e. shaft). These implants typically have a tight fit between the polyethylene post and femoral box which can provide knee stability in the setting of damaged ligaments.

Hinged Knee Implants
Hinged knee implants are used in cases of severe bone loss or ligament damage. These implants can be used to treat tumor resections, massive fractures in elderly patients and knees that have already been revised multiple times. Hinged knee implants will often have a bar that locks into the femoral component that allows flexion and extension. The tibial component will often have a central post that allows internal and external rotation (i.e. rotating hinge). These implants have the highest constraint so they put more force on the implant to bone interface, which lead to slightly higher early failure in older hinged knee designs. Current design have improved the implant to bone interface and makes these implants a reasonable solution for a bad problem.
Press Fit vs. Cemented fixation

Press Fit Fixation
Press fit implants have a porous coating on the bone facing side such that the patient’s bone can grow into the implant. These implants have a slightly higher early failure rate and a lower late failure rate. Once the bone is ingrown, the implant should be well attached to the bone for life. Surgeons must be meticulously when preparing the bone for a press fit implant, so that the saw blade does not burn the bone and kill the bone cells.
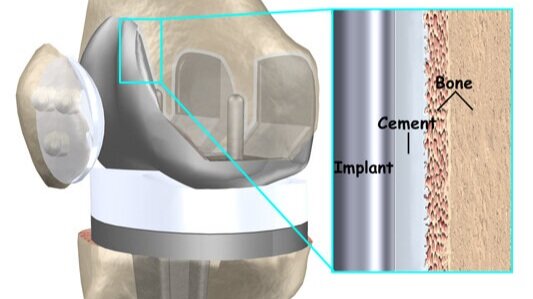
Cemented Fixation
Bone cement is typically used to bond the implant to the bone. When the monomer and polymer are mixed, bone cement feels like cookie dough and hardens in about 5-10 minutes. The cement fills in the cracks and crevices of the bone and firmly fixes the implant to the bone. These implants have little pockets on the back of the implants where the bone cement can reside to help improve fixation. Bone cement does not have any adhesive properties. If a knee replacement is mal-aligned, or grossly unstable, the implant can loosen from the bone cement.